But hey, it's MVP...
Apr 09, 2024
I hear it often -- "We need an MVP." But most of the time it really means, we need a prototype on the cheap. Or, we need to get our first product launched and we're operating on a shoestring.
Funds are tight (especially right now in MedTech), but this interpretation of MVP is way off. And the shortcut strategy is flawed too. Let me explain why.
But first.. if you aren't familiar, MVP = Minimum Viable Product. It's all the rage in startup circles. Born in the software world, it's migrated into consumer products, and it now lives in MedTech too.
At its core, MVP is about testing assumptions. Some assumptions, like willingness to pay, are universally hard to test until the product is actually ready to buy. Asking prospects "what would you pay for this?" generates completely unreliable data.
So, what has this led teams to do? In many cases, lock engineers in the lab until they come out with a solution. And, sometimes (often) it looks like the image above.
Now maybe the tech is amazing. And maybe there've been great scientific advancements. But almost all the time, this heads-down approach results in a product that is completely misaligned with the adoption drivers of customers. Medtech-market mismatch. Gut punch.
But hey, it's MVP..
Now we pivot.. Right?
Yep, a pivot indeed. But a really expensive one. Fixing problems later always costs more (much more) than fixing problems earlier in development. Reworking tooling, redoing V&V, rerunning clinicals.. The spend to fix is at least 2X the spend to do it right the first go round.
Then comes the axe: "Scrap it. Fire the CEO. Hire a more seasoned management team. Reboot," says the board. A terrible outcome for founders, early investors, and often employees associated with the original (flawed) MVP approach.
But is MVP all wrong?
I don't think so. At it's core, MVP is about lining up and knocking down the killer assumptions. And while it makes little sense in MedTech to assess all these assumptions together in final device form, there are fast and effective ways of applying MVP thinking early in development -- keeping the costs of change low.
The key is to reframe what MVP means in MedTech. It's still about testing assumptions. And the biggest assumption will forever be, "Will Customers Buy?" The MVP reframing comes down to: what is it that customers are actually buying in healthcare?
We all think that customers in MedTech are buying devices. Duh, right? But that's actually not the case. MedTech customers (the ones writing the checks) don't give two bits about the device itself.
They care about what the device does. They care about the clinical outcomes - incidence of procedural complications, rates of infection, disease exacerbation, recurrence of symptoms, mortality rates. These are the kinds of outcomes that affect patient lives, hospital reputations, and quality scores. These are the kinds of clinical outcomes that could be improved by your promising new medical device.
But just as important these days are the economic outcomes. Hard to get hospitals to change without pulling the money levers. Reduced length of stay, improved readmission rates, reduced absorbed procedure costs, increased procedure profit. These are the economic drivers that drive hospitals to buy. And hopefully these economic drivers can also be improved by your medical device. Able to improve both clinical and economic stories? Double points.
Again, healthcare customers aren't buying devices; they're buying outcomes. So, your MVP represents the outcomes that will may your customer to buy.
MVP = Outcomes
Back to MVP basics -- it's about testing critical assumptions. So, if we now think of your MVP as the outcomes that will drive your customers to buy, then what assumptions do we have about these outcomes?
Some possible assumptions..
- The outcome relates to a high priority problem for your customer.
- The customer measures the outcome the same way you do.
- Your customer is willing to incur the change needed to obtain your promised outcome.
Let's dig into that last assumption for a sec -- justifying change.
Say you have a new type of urinary catheter, one that promises to reduce the rate of urinary tract infections (UTIs) in the hospital by approximately 10%. However, this new device requires some operational changes for the nursing staff to use it properly.
Urinary catheters are a high volume device used throughout the hospital. Nursing is in the mode of efficiently applying and managing the standard devices, Foley catheters. Introducing a new type of catheter is going to affect workflow -- no doubt about it. Doesn't mean that it can't be done, but it will require some effort.
Think about it this way:
- All the nurses will need to be retrained on the new catheter
- There may be larger inventory needed, since the new catheter won't replace all Foleys in use
- New contracts need to be set up; perhaps new negotiations with group purchasing organizations (GPO) for these high volume supplies
- Surveillance may be introduced to evaluate the effectiveness (and side-effects) of the new device after it's put in-use
That's a high effort to the hospital for what seems like it should be a relatively simple swap. It's not as simple as just buying a new device and putting it to use.
And this is a big part of reason for value analysis committees -- is the clinical and economic upside (impact) high enough to justify the costs of change (effort)?
Think of it like this chart:
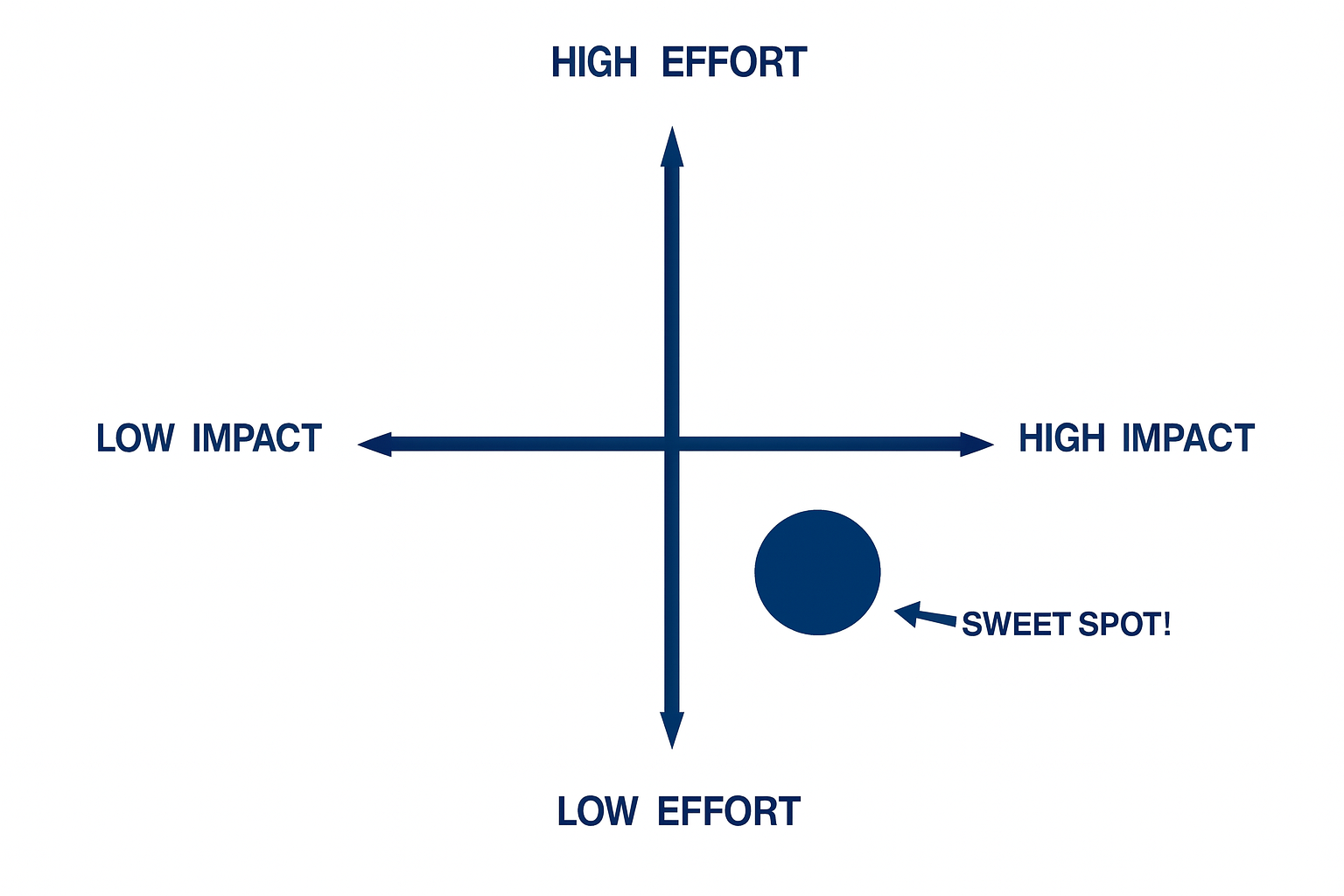
Healthcare is like a giant flywheel. It has a tremendous amount of momentum -- wants to keep going and going in the same direction. It's rare to get that flywheel to stop and change directions. Better to figure out a way to keep it flying in the same direction with minimal resistance.
In the urinary catheter example above, the changes to workflow, training, supply chain may push the required customer change into the high effort side of the plot.
But what about the benefits -- the positive impact? 10% improvement may be considered a modest improvement. This impact is probably living in the low impact side of the plot.
That's not a winning combination -- high effort, low impact.
In this short UTI example, how can we shift things into the low effort, high impact quadrant? That's the sweet spot. Maybe there are design changes that need to be introduced to minimize workflow changes required? Maybe there's a subpopulation that this device can provide a much greater UTI incidence improvement?
It's better to zoom in on a smaller population that puts you in the low-effort, high-impact quadrant than stick with a monster (general) market that keeps you in the high-effort, low-impact quadrant.
So what does this all have to do with MVP?
Remember, your MVP is the outcome that matters to customers (not the device). Now, use that outcome to help assess your assumptions. Some of those assumptions relate to impact versus effort, as discussed above. Your job now is to test those assumptions in the most efficient way possible - the Minimum Viable way.
Is this minimum viable way to build tech, run preclinical/clinical tests, document the results? Is it to create high fidelity prototypes that you can pitch to physicians and nurses?
Definitely not. Those methods focus on the device, not the outcomes. Testing the outcomes can be achieved much more simply through the following:
- Conversations with nurses and physicians to understand how they think about your proposed clinical outcomes (high versus low impact)
- Workflow studies to understand the standard of care and potential change to the standard of care (high versus low effort)
- Healthcare economics analyses to compare the baseline costs and the economic improvements you expect your customers to gain (high versus low impact)
This type of MVP thinking is way different than the cheap prototype MVP you may have had in-mind. But it's a better way to MVP. It will force you to focus on the actual drivers for adoption and the resistance that you're likely to face down the road.
And when you gain these insights around adoption (early), you'll have the data to make better decisions around your market strategy. That's what should drive everything else -- your labeling, your regulatory pathway, your product design, your manufacturing methods. It all starts with a clear understanding of the user, customer, and market needs.
That's what MVP can do for you, when you reframe it the right way.
To sum it up..
MedTech MVP = The critical outcomes that matter to your customers
Key Assumption = Positive impacts outweigh customer efforts
Early Tests = Candid conversations and analyses
A 360⁰ MedTech Audit now could avoid a major disaster later.
You may be on the right path in MedTech. But there could be some gaps, some blind spots, some issues that pop up later when the costs of change could sink the ship.
Wouldn't it be better to get in front of them now?
If so, let's discuss a 360⁰ MedTech Audit. We'll dig into your market strategy, clinical strategy, regulatory strategy, IP strategy, product development strategy, and all of the intricacies between them.
It's a small insurance policy that could avoid a huge amount of time, budget, and frustration down the road. What's stopping you?
Just contact us to explore.
Eric Sugalski
Founder
Support for MedTech at Every Stage
Archimedic partners with medical device teams to solve complex design, development, regulatory, and go-to-market challenges.